|
11/2/2020 0 Comments Severe Asthma Management in the ED
Therapy Options:
0 Comments
9/9/2020 0 Comments Bradycardia Basics
7/30/2019 0 Comments Skin and Soft Tissue Infections
Skin and Soft Tissue Infections
Epidemiology
Important Aspects of your History
The Mimics
Workup
Treatment
“Special” cellulitis
Necrotizing fasciitis +/- Toxic Shock Syndrome
Republished with Permission from www.PedEMMorsels.com
Difficult Airway: Basics
Difficult Airway: Important Differences Anatomic and physiologic differences influence how the oral, pharyngeal, and tracheal axes align as well as how the respiratory mechanics function and how the child compensates to physiologic stress. The differences are most prominent in children < 2 years of age and more adult anatomy evolves as children progress to 8 years of age. Anatomic Differences:
Physiologic Differences:
Difficult Airway: Predictive Factors
Difficult Airway: Assume the Worst
Moral of the Morsel
Taking care of children in the ED isn't just diagnosing viruses - child abuse/neglect is more prevalent than we'd like to think:
- 2-10% of children presenting to the ED are victims of abuse or neglect - children that are abused often have multiple healthcare visits before it is recognized Child maltreatment includes neglect and abuse Neglect - failure to meet the most basic needs of a child (food, shelter, supervision, nurturance) - can be educational, psychological, emotional, medical neglect, or supervisory - by far the most common type of maltreatment - about ⅔ of cases - very difficult to identify diagnose Abuse - includes physical abuse, sexual abuse, emotional abuse, and medical child abuse * medical child abuse is the current term for Munchausen Syndrome by proxy - physical abuse (also referred to as non-accidental trauma or NAT) is often the most recognizable type of abuse - makes up 16% of maltreatment cases Providers should be mindful of sentinel injuries - injuries without a plausible explanation - knowing basic developmental milestones can be helpful 4-5 months - rolling over 6 months - sitting unassisted 9 months - pulling to a stand and walking 12 months - walking **soft tissue injuries - bruising in children who cannot cruise, or in high risk areas - normal childhood bruises occur on surfaces that take impact when the child falls bruising on the knees and shins isn’t alarming bruising on areas like the back, buttocks, thighs, abdomen is concerning - TEN-4 FACES P can help you identify injuries that suggest potential abuse * bruising on the Trunk, Ears, or Neck in a child less than 4 years old * ANYbruising on a child less than 4 months * injuries/bruising to the Frenulum, Auricular area, Cheek, Eyes, Sclera or * Patterned bruising is a red flag **skeletal injuries are the second most common presentation of abuse - certain fractures should raise your suspicion for abuse - rib fractures (make sure you check that CXR ordered to look for pneumonia) - any fracture in a child that cannot walk - long bone fractures in an infant or toddler **abusive head trauma (formally known as “shaken baby syndrome”) - this is the most common cause of death following abuse - 30% of cases are missed initially – remember to consider it in cases of excessive fussiness or altered mental status **chest and abdominal injuries - the abdomen can hide injuries and hold a lot of blood - you won’t always see bruising - elevated liver enzymes or lipase should raise your concern for occult intra-abdominal injury What can you do to help prevent a missed diagnosis of abuse?
ACEP Now. The Recognition of Child Abuse. May 1, 2012. Colbourne M, Clarke MS. Child Abuse and Neglect. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e New York, NY: McGraw-Hill; 2016. http://accessmedicine.mhmedical.com.libproxy.lib.unc.edu/content.aspx?bookid=1658§ionid=109435341. Accessed May 15, 2019. Christian CW. The Evaluation of Suspected Child Abuse. PEDIATRICS. 2015; 135 (5): e1337-e1354. Glick JC, Lorand MA, and Bilka KR. Physical Abuse of Children. Pediatrics in Review. 2016; 37(4): 146-158. Lindberg DM, Beaty B, Juarez-Colunga E, et al. Testing for Abuse in Children With Sentinel Injuries. PEDIATRICS. 2015; 136(5): 831-838. Petska HW and Sheets LK. Sentinel Injuries Subtle Findings of Physical Abuse. Pediatric Clinics of North America. 2014; 61(5): 923-935. Ravichandiran N, Schuh S, Bejuk M, et al. Delayed Identification of Pediatric Abuse-Related Fractures. PEDIATRICS. 2009; 125 (1): 60-66. Sheets LK, Leach ME, Koszewski IJ, et al. Sentinel Injuries in Infants Evaluate for Child Physical Abuse. PEDIATRICS. 2013; 131(4): 701-107. Teeuw AH, Derkx BHF, Koster WA, et al. Detection of child abuse and neglect in the emergency room. European Journal of Pediatrics. 2012; 171: 877-885. Teeuw AH, Hoytema van Konijnenburg EM, Sieswerda-Hoogendoorn T, et al. Parents’ Opinions About a Routine Head-to-Toe Examination of Children as a Screening Instrument for Child Abuse and Neglect in Children Visiting the Emergency Department. Journal of Emergency Nursing. 2016; 42(2): 128-138. 3/22/2019 0 Comments Myasthenic Crisis
MG Pathophysiology & Symptoms
MG Crisis (MC) Causes
Drugs to avoid in MG Patients:
Drugs that should be used with caution:
Evaluation
Focused 30-second Neuro Exam
Airway Management
- Vital capacity less than 10-20 mL/kg - Single-breath test (unable to count past 20) - Unable to clear secretions
Management After Stabilization
Sources: Bird, S.J. & Levine, J.M (2019). Myasthenic crisis. In A.F. Eicheler & G. Finlay (Ed.), UpToDate.Retrieved February 27, 2019, from https://www.uptodate.com/contents/myasthenic-crisis Howard, J.F. (2009). Myasthenia Gravis: A manual for the health care provider. Myasthenia Gravis Foundation of America, Inc. Jowkar, A. (2010). Neuromuscular topics for Neuroscience ICU RNs. Presentation, University of North Carolina at Chapel Hill. Roper, J., Fleming M.E., Long. B. et al. (2017). Myasthenia Gravis and Crisis: Evaluation and Management in the Emergency Department. The Journal of Emergency Medicine, 53(5): 843-853. http://dx.doi.org/10.1016/j.jemermed.2017.06.099 Tintinalli, J. E., Stapczynski, J. S., Ma, O. J. et al. (2016). Tintinalli's emergency medicine: A comprehensive study guide(Eighth edition.). New York: McGraw-Hill Education. 2/8/2019 0 Comments Vasopressors in the ED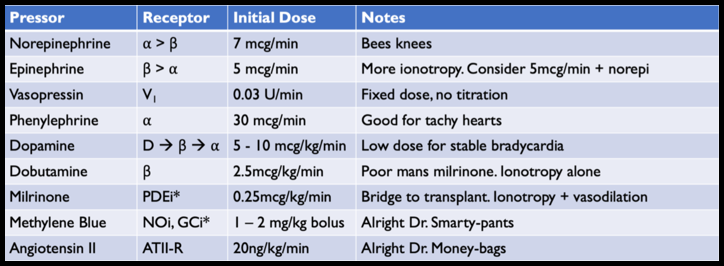
ED Vasopressors – Core Concepts
Our body has 3 major classes of vasopressors - Catecholamines - ⍺/β receptor agonism - Vasopressin – Vasopressor receptor (V1) agonism - Angiotensin II – Angiotensin II Receptor (ATII-R) agonism We use vasopressors to supplement our bodies own mechanisms to increase blood pressure. VASOPRESSOR AGENTS Norepinephrine ONE LINER: THE “BEES KNEES” OF VASOPRESSORS - Mechanism: ⍺/β agonism - Dose: Initial dose 5mcg/min (0.05mcg/kg/min) - Indication: Any shock, the best agent in (ALMOST) all circumstances: SOAP II (NEJM 2010) – Norepi vs dopamine for shock (primarily sepsis); Levy et al (JACC 2018) – Norepi vs epi for post AMI cardiogenic shock; VASST (NEJM 2008) – More norepi vs norepi + vasopressin - Good/bad: (+) Literally the best, (+) Safe for peripheral administration, (-) Can cause arrhythmias Epinephrine ONE LINER: NOT AS GOOD AS NOREPI, MAY HELP A DYING HEART - Mechanism: β/⍺ agonism - Dose: Initial dose 5mcg/min (0.05mcg/kg/min) - Indication: Hypotension + bad heart – hypotension AND bradycardia; hypotension with poor contractility (titrate epi for heart function on POCUS + titrate norepi for BP); Periarrest phase (push-dose epi) - Good/bad: (+) Give a dying heart a better chance (maybe); (+) Can be used in push dose; (-) Lactate no longer reliable for monitoring shock; (-) Increased arrhythmias; (-) Limited evidence that epi is superior to norepi in most situations Phenylephrine ONE LINER: USE FOR IATROGENIC HYPOTENSION OR FOR A FAST HEART - Mechanism: Pure ⍺ - Dose: Initial dose 50mcg/min (0.5mcg/kg/min) - Indication: Sedation induced hypotension, hypotension with arrhythmia (Afib with RVR) - Good/bad: (+) Not arrhythmogenic; (-) Bad in heart failure Dopamine: ONE LINER: POOR MAN’S NOREPI - Mechanism: Dopa/β/⍺ agonism - Dose: Dose dependent effects o Low Doses: 2 – 5 mcg/kg/minàDopa agonismo Mid Doses: 5 – 10 mcg/kg/minàβ agonism o High Doses: 10 – 20 mcg/kg/minà⍺ agonism - Indication: Bradycardia OR Hypotension. If both, use epi - Good/Bad: (-) Arrhythmias; (-) More adverse events compared to norepi Vasopressin: ONE LINER: SUPPLEMENTAL VASOPRESSOR, NEVER AS A SINGLE AGENT - Mechanism: Vasoconstriction via Vasopressin (V1) receptor - Dose: Fixed dose 0.03U/min, no titration. Can use 20U as single bolus in cardiac arrest with steroids (VSE 2013) - Indication: Shock (septic, vasodilatory), renal failure - Good/bad: (+) No adrenergic activity – no arrhythmias, does not compete with catecholamines (+) Maybe decrease need for dialysis compared to norepi (VANISH Trial). (-) No mortality benefit compared to Norepi THE OTHER AGENTS: Almost never used in ED Dobutamine: - Mechanism: β agonism, no ⍺ - Indications: Bradycardia, cardiogenic shock - Dosage: Start at 2.5 mcg/kg/min (Max 20mcg/kg/min) - Notes: Poor-mans milrinone. (-) Bad dysrhythmias. (+/-) Not a true “pressor”; Can cause vasodilation via β2 without ⍺ activity Milrinone: - Mechanism: PDE inhibitor o Increased [Ca]i via cAMPàIonotropy + vasodilation o Lusitropiceffects–Increaseddiastolicrelaxation/filling o IncreasedPreload+Increasedcontractility+decreasedSVR=IncreasedCO - Indications: Heart failure (with goals of transition to either transplant or assist device) - Dosage: 0.25 – 0.5 mcg/kg/min - Notes: (-) Causes arrhythmias. (+/-) Vasodilator. Needs continuous infusion through PICC Methylene Blue: - Mechanism: Inhibit NO/cGMP vasodilation - Indications: Refractory vasodilatory shock - Dosage: 1-2mg/kg as bolus over 15min; Infusion 0.5mg/kg/hr x 4hrs - Notes: Used for refractory hypotension, used for salvage therapy Angiotensin II - Mechanism: Binds Angiotensin-II receptors for direct vasoconstriction - Indications: Refractory vasodilatory shock - Dose: Start at 20ng/kg/min (Max 200ng/kg/min) - Notes: Hasn’t been looked at as solo vasopressor, just for refractory shock with other agents. - Very expensive without mortality benefit (ATHOS-3) |
 RSS Feed
RSS Feed
LEGAL DISCLAIMER (to make sure that we are all clear about this):The information on this website and podcasts are the opinions of the authors solely.
For Health Care Practitioners: This website and its associated products are provided only for medical education purposes. Although the editors have made every effort to provide the most up-to-date evidence-based medical information, this writing should not necessarily be considered the standard of care and may not reflect individual practices in other geographic locations.
For the Public: This website and its associated products are not intended to be a substitute for professional medical advice, diagnosis, or treatment. Your physician or other qualified health care provider should be contacted with any questions you may have regarding a medical condition. Do not disregard professional medical advice or delay seeking it based on information from this writing. Relying on information provided in this website and podcast is done at your own risk. In the event of a medical emergency, contact your physician or call 9-1-1 immediately.
For Health Care Practitioners: This website and its associated products are provided only for medical education purposes. Although the editors have made every effort to provide the most up-to-date evidence-based medical information, this writing should not necessarily be considered the standard of care and may not reflect individual practices in other geographic locations.
For the Public: This website and its associated products are not intended to be a substitute for professional medical advice, diagnosis, or treatment. Your physician or other qualified health care provider should be contacted with any questions you may have regarding a medical condition. Do not disregard professional medical advice or delay seeking it based on information from this writing. Relying on information provided in this website and podcast is done at your own risk. In the event of a medical emergency, contact your physician or call 9-1-1 immediately.